ENERGY ENHANCEMENT ALCHEMICAL VITRIOL THE GROUNDING OF NEGATIVE ENERGIES AND THE ROSS TRAUMA MODEL OF MENTAL DISORDERS
ENERGY ENHANCEMENT EASY EFFECTIVE ENLIGHTENMENT
TRAUMA MODEL DIRECTORY
Post-traumatic Stress Disorder (PTSD) Nervous Breakdown UNSTOPPABLE EMOTIONS AND GROUNDING THESE NEGATIVE ENERGIES ENERGY ENHANCEMENT ALCHEMICAL VITRIOL THE GROUNDING OF NEGATIVE ENERGIES AND THE TRAUMA MODEL OF MENTAL DISORDERS
AN ENERGY ENHANCEMENT REVIEW OF THE TRAUMA MODEL - Childhood trauma, psychosis and schizophrenia:- a review of the current 2004 literature with theoretical and clinical implications
THE TRAUMA CREATION OF ENERGY BLOCKAGES
"An example of one of the different types of Energy Blockage
is that they are sometimes created when we do not get what we expect, or we get what we do not want. They are caused by the Trauma of Disappointment.Like when our Mother or Father or Son or Daughter dies. Like when a Lover leaves us.
This trauma, this pain is so strong that at that moment the mind can not look at it, so it gets locked away within the body until we get strong enough to process it.
Then amnesia. We forget the pain fulminating in our bodies. We forget the poison until, after a while, disease is the result."
Satchidanand
Energy Enhancement experience agrees with the Psychological Trauma Model, yet Energy Enhancement goes further in two ways...
1. ENERGY ENHANCEMENT TECHNIQUES GROUND TRAUMA - The solution to psychological symptoms caused by trauma is the Third Initiation of Level One of Energy Enhancement - The Grounding of Negative Energies. It is based upon ancient meditational techniques successfully used to create Enlightened People for over Five Thousand years. All successful initiates have overcome all Trauma Caused Energy Blockages in order to become enlightened. Indeed Enlightenment is the only psychological model ending in a total cure of all psychological problems.
Enlightenment - a total cure of all psychological problems - the removal of all pain and the promotion of peace, is based upon the Grounding of Negative Energies which is one part of the Kundalini Kriyas and the Taoist Meditational Orbits. The Grounding of Negative Energies is also based upon VITRIOL Theory and the Chakras originally based upon Four Thousand years old Taoist Acupuncture, Taoist Alchemy leading on to the Alchemical VITRIOL Theory based upon its entrance into Europe in the Middle Ages in Latin.
VITRIOL - Visita Interiora Terrae Rectificando Invenies Occultem Lapidem is the first formula or Guided Meditation of Alchemy. It gives a methodolgy to remove all trauma formed negative Energies from the psychic system. It always works. It always works better than just talking about the problem as is the case in Psychiatry.
The Raja Yoga of Patanjali for five thousand years has always been the method of choice to get to that symptomless state of Peace, Love and Illumination.
FREE VIDEO DOWNLOAD FOR ENERGY ENHANCEMENT SOUL FUSION AND THE
SUPRA-GALACTIC ORBIT - PLAY IN WINDOWS MEDIA PLAYER..
http://bit.ly/h7lRlJ
FREE ENERGY ENHANCEMENT VITRIOL DOWNLOAD - CLICK HERE TO SAVE THE
WHOLE VITRIOL VIDEO ON YOUR COMPUTER!! - PLAY IN WINDOWS MEDIA
PLAYER..
http://bit.ly/ih01y5
2. EVERYONE HAS THE SYMPTOMS OF TRAUMA - Most people are not enlightened therefore most people have psychological symptoms which are the root cause of all problems in their lives, the difference being in the degree of Trauma given in the various ages of life - the more trauma, the more problematic the symptoms. Yet although in most people the trauma is less, still this trauma causes all the problems of life.
ENERGY ENHANCEMENT CHAKRAS DIRECTORY - CHAKRAS ABOVE THE HEAD, CHAKRAS IN THE BODY AND CHAKRAS BELOW THE BASE CHAKRA - THE ANTAHKARANA
ENERGY ENHANCEMENT ENERGY BLOCKAGE DIRECTORY - ENERGY BLOCKAGES ARE CREATED FROM TRAUMA FORMED NEGATIVE KARMIC MASS - ENERGY BLOCKAGES ARE PURE CONCENTRATED EVIL WHICH BLOCK US OFF FROM THE SPIRIT
THE ENERGY ENHANCEMENT KUNDALINI KRIYAS DIRECTORY -
KRIYA YOGA AND THE TAOIST ORBITS COME FROM CIRCULAR ENERGY FLOWS IN THE GOVERNING AND CENTRAL MERIDIANS WHICH WHEN USED CAN REMOVE BLOCKAGES IN THOSE MERIDIANS AND ALL CHAKRASENERGY ENHANCEMENT ANTAHKARANA DIRECTORY - THE ANTAHKARANA IS THE REAL GOLDEN ROD AND VERTICAL CENTRAL PILLAR OF THE ALCHEMISTS - IT IS THE PSYCHIC CONSTRUCTION BETWEEN HEAVEN AND EARTH WHICH SHOWS HOW HUMANITY CONNECTS WITH THE ASTRAL PLANE AND WITH GOD - IT IS THAT WHICH MUST BE BLOCKED IN ORDER TO CONTROL HUMANITY
THE ENERGY ENHANCEMENT SAMADHI SAMYAMA DIRECTORY - SAMADHI AND SAMYAMA ARE THE EIGHTH AND NINTH LIMBS OF YOGA OF RAJA YOGA AS SPECIFIED IN THE SOURCE BOOK, THE YOGA SUTRAS OF PATANJALI WHICH GIVES THE METHODOLOGY - THE TECHNIQUES - FOR THE REMOVAL OF ENERGY BLOCKAGES AS A PRELUDE TO KAIVALYA ILLUMINATION - COMMENTARY ON THE YOGA SUTRAS BY SATCHIDANAND HERE!!
ENERGY ENHANCEMENT EMOTIONAL BLOCKAGES DIRECTORY
EMAIL sol@energyenhancement.org for details
THE TRAUMA MODEL
Trauma models of mental disorders (alternatively called trauma models of psychopathology) emphasize the effects of psychological trauma, particularly in early development, as the key causal factor in the development of some or many psychiatric disorders (in addition to post-traumatic stress disorder).
Trauma models are typically founded on the view that traumatic experiences (including but not limited to actual physical or sexual abuse) are more common or more serious than thought in the histories of those diagnosed with mental disorders. Such models have traditionally been associated with psychoanalytic approaches, notably Sigmund Freud's early ideas on childhood sexual abuse and hysteria.
John Bowlby, who developed attachment theory, also describes many forms of mental illness as based on early childhood trauma.[1] In addition there is significant research supporting the linkage between early experiences of chronic maltreatment and later problems.[2]
In the 1960s trauma models also became associated with humanist and anti-psychiatry approaches, particularly in regard to understanding schizophrenia and the role of the family.[3] Personality disorders have also been a focus, particularly borderline personality disorder. Extreme versions of trauma models have implicated the fetal environment and the trauma of being born, or have been associated with recovered memory controversies.
More generally, trauma models highlight particularly stressful and traumatic factors in early attachment relations and in the development of mature interpersonal relationships. They are often presented as a counterpoint to a psychiatry claimed to be too focused on genetics, neurochemistry and medication.
Contents |
History
In the 1940s, '50s, '60s and '70s some mental health professionals proposed trauma models to understand schizophrenia: Harry Stack Sullivan, Frieda Fromm-Reichmann, Theodore Lidz, Gregory Bateson, Silvano Arieti, R.D. Laing and others. They held that schizophrenia is induced by traumatic experiences in profoundly disturbed families, or by attempts to cope with a tramatically damaging society. In the 1950s Sullivan's theory that schizophrenia is related to traumatic interpersonal relationships was widely accepted in the United States.
The Diagnostic and Statistical Manual of Mental Disorders, or DSM, does not claim that the specific etiology of schizophrenia and other serious psychoses has been established. However, the psychogenic models proposed by these early researchers are no longer in vogue in the psychiatric profession. Since the 1960s pharmacological treatments became the increasing focus of psychiatry, and by the 1980s the theory that the family dynamics could be implicated in schizophrenia became a taboo in many quarters.[4]
Before his death in 2001, aged ninety, Lidz, one of the main proponents of the "schizophrenogenic" parents theory, expressed regret that current research in genes biological psychiatry is "barking up the wrong tree".[5] Correlation of schizophrenia in genetic twins in only 30% - trauma is a more4 likely cause. Like Lidz, Laing maintained until his death that the cause of both schizoid personalities and schizophrenia was influenced by traumatic family relationships.
In 1975 Silvano Arieti won the American National Book Award in the field of science for his book, Interpretation of Schizophrenia, which advances a psychological model for understanding all the regressive types of the disorder.[6] This idea has been superceded- according to more recent research, traumatic child abuse at home plays a more causal role in depression, PTSD, eating disorders, substance abuse and dissociative disorders.[7]
The more severe the traumatic abuse the more probability symptoms will develop in adult life.[8] In the psychiatric field it is hypothesized that child abuse is less related to the most serious psychoses, such as schizophrenia.[verification needed] However, some mental health professionals maintain that the relationship is stronger in psychoses than neuroses.[9]
In a study of 150 people under sentence of death in the USA, 100% of the people had been severely traumatised by sexual and physical abuse.
Psychohistory table
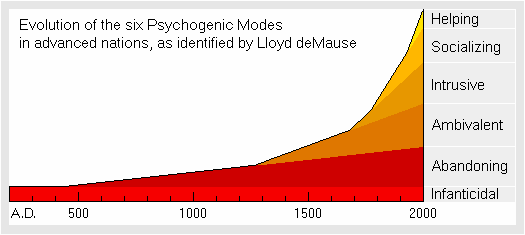
The chart below shows the dates at which gradual forms of child abuse are believed by psychohistorians to have evolved in the most advanced nations, based on accounts from historical records. The timeline doesn't apply to hunter-gatherer societies. It doesn't apply either to the Greek and Roman world, or the ancient Chinese world where there was a wide variation in childrearing practices. The major childrearing types described by Lloyd deMause are:
With the exception of the "helping mode of childrearing" (marked in yellow above), for psychohistorians the major childrearing types are related to main psychiatric disorders, as can be seen in the following Table of Historical Personalities:
| Childrearing | Personality | Historical Manifestations |
|---|---|---|
| Infanticidal | Schizoid | Child sacrifice and infanticide among tribal societies, Mesoamerica, the Incas; in Assyrian and Canaanite religions. Phoenicians, Carthaginians and other early states also sacrificed infants to their gods. On the other hand, the less abusive Greeks and Romans exposed some of their babies to death. |
|
Narcissistic |
||
| Abandoning | Masochistic | Longer swaddling in the early Middle Ages, fosterage, outside wetnursing, oblation of children to monasteries and nunneries, and apprenticeship. |
| Ambivalent | Borderline | Although the later Middle Ages ended the abandonment of children to monasteries, "ambivalent" parents tolerated extreme love and hate for the child without the two feelings affecting each other. Enemas, early beating, shorter swaddling, mourning for deceased children, a precursor to empathy. |
| Intrusive | Depressive | The intrusive parent began to unswaddle the infant. Since infants were now allowed to crawl rather than being swaddled, they had to be formally traumatically "disciplined", threatened with hell; use of guilt. Early toilet training, repression of child's sexuality, end of swaddling and wet-nursing, empathy now possible, rise of pediatrics. |
| Socializing | Neurotic | Use of "mental discipline"; teaching children to conform to the parents goals, socializing them. Hellfire and physical discipline disappeared. Rise of traumatic compulsory schooling. The socializing mode is still the main mode of upbringing in the West. |
| Helping | Individuated | Absolute end of humiliation to control the child. The helping parent tries to assist the child in reaching its own goals rather than socializing him or her into adult goals. Children's rights movement, deschooling. |
Recent approaches
In more recent years psychologist Alice Miller, author of twelve books on mental distress and disorders, including non-psychiatric conditions like falling prey to cults, has informed future parents and former victims about the disastrous consequences of child abuse. Former schizophrenic patients, such as John Modrow, have also endorsed the views of the pioneers of the trauma models.[13]
The "trauma model of mental disorders" is the name given by psychiatrist Colin A. Ross to his specific model, which is presented as a solution to the problem of comorbidity in the mental health field.[14]
Comorbidity - In psychiatry, psychology and mental health counseling comorbidity refers to the presence of more than one diagnosis occurring in an individual at the same time. However, in psychiatric classification, comorbidity does not necessarily imply the presence of multiple diseases, but instead can reflect our current inability to supply a single diagnosis that accounts for all symptoms.[2] On the DSM Axis I, Major Depressive Disorder is a very common comorbid disorder. The Axis II personality disorders are often criticized because their comorbidity rates are excessively high, approaching 60% in some cases, indicating to critics the possibility that these categories of mental illness are too imprecisely distinguished to be usefully valid for diagnostic purposes and, thus, for deciding how treatment resources should be allocated.
An information packet given to inpatients at the Ross Institute for Psychological Trauma describes the theoretical basis of his trauma model in commonsensical terms:
| � | The problem faced by many patients is that they did not grow up in a reasonably healthy, normal family. They grew up in an inconsistent, abusive and traumatic family. The very people to whom the child had to attach for survival, were also abuse perpetrators and hurt him or her badly [...] The basic conflict, the deepest pain, and the deepest source of symptoms, is the fact that mom and dad's behavior hurts, did not fit together, and did not make sense. | � |
The Trauma Model A
Solution to the Problem of Comorbidity in Psychiatry By: Colin A.
Ross, M.D.
Twenty-one years ago, in 1979, I did my clinical rotation in
psychiatry as a medical student at the University of Alberta, in
Edmonton, Canada. I noticed then that psychiatric inpatients tended
to have many different diagnoses. They would be admitted and treated
for depression on one occasion, and for a psychotic disorder another
time, and often would have numerous admissions. The current
diagnosis was always the correct one, but at some point in the
future it would become a past incorrect diagnosis. I was most
troubled when I saw the diagnosis change several times in a single
admission. Not uncommonly, the diagnosis was changed in order to
provide a rationale for prescribing a new medication.
Some psychiatrists were simply sloppy diagnosticians and irrational
polypharmacists. Others were careful, conscientious and reasonable.
The problem was that the patients did not fit the conceptual system
of late twentieth century psychiatry. Even when the conceptual
system was applied consistently, it did not work. The patients were
too polymorphous, variable, complicated and, often, uncooperative. I
was taught that sometimes this was because the patient was
"borderline." Borderlines, I was taught, display pan-anxiety,
pan-sexuality, and polymorphous perversity. Those terms conveyed to
me the frustration generated by the conceptual system.
Even if the "borderline" patients were set aside, the problem
persisted. On the inpatient wards, the norm was extensive
comorbidity. I have been thinking about this problem for twenty-one
years, and have devised a solution for it, which I call the trauma
model. The purpose of this book is to define the problem of
comorbidity, and then to describe its solution through the trauma
model. The trauma model is a comprehensive, testable scientific
theory of mental illness.
The polydiagnostic patient with extensive comorbidity is the major
recipient of inpatient psychiatric treatment. In managed care terms,
this is the high-cost, high-utilization, high-recidivism patient.
There is no scientific model in psychiatry which accounts for this
patient, even though he or she is the major consumer of psychiatric
services. The dominant model in contemporary psychiatry is the
single gene-single disease model. Insurance policies which have
expanded their coverage for serious mental illness include disorders
assumed to be distinct genetic biomedical brain diseases within
contemporary psychiatry; schizophrenia, unipolar and bipolar
depression, obsessive-compulsive disorder, and substance abuse.
Yet, the patients requiring expensive psychiatric care, for the most
part, do not fit the single gene-single disease model. They meet
DSM-IV-TR (American Psychiatric Association, 2000) criteria for many
different disorders and are often given many different clinical
diagnoses over time. The separate diseases model simply cannot
account for the clinical data. The problem of comorbidity, from a
financial perspective, is the core clinical problem in psychiatry.
The solution for the problem of comorbidity adopted by psychiatry
over the next ten years will set the tone for research, theory,
clinical practice and health care coverage in the twenty-first
century. In this book, I propose the trauma model as a
scientifically testable solution to the problem of comorbidity.
In the first section of the book, the clinical origins and a formal
scientific statement of the problem of comorbidity are presented. In
the second section, key assumptions of the model are outlined in
detail. The third section begins with a description of some general
principles of the model, then takes up each of the major sections of
DSM-IV-TR. In each of these chapters I describe the specific
research predictions arising from the trauma model. These are
divided into subsections on phenomenology, natural history,
epidemiology, twin and adoption studies, biology, treatment outcome,
and revisions to DSM-IV-TR.
In the fourth section of the book, trauma therapy is described. The
basic principles and techniques in the psychotherapy of the
extensively comorbid patient are outlined. These tend to be
cognitive-behavioral in form. As in the rest of the book, the
therapy is grounded in relevant bodies of science wherever possible.
The testability of the therapy is dealt with in the separate
chapters of the previous section.
In the final chapter, the trauma model is discussed from the
perspective of the structure of scientific revolutions (Kuhn, 1962).
Adoption of the trauma model by mainstream psychiatry would
represent a major paradigm shift. At present, the trauma model is
marginalized and has no impact on the majority of research, clinical
practice and theory in psychiatry. This fact presents an interesting
opportunity for anyone interested in scientific paradigm shifts.
Major paradigm shifts do not occur every decade in a given field, or
even every century. Here we have one in progress. Or, alternatively,
one that will fail. Either way, the fate of the trauma model will
provide interesting lessons about the balance of science and
politics in psychiatry.
I have made no effort to be comprehensive in my references because
there is no point. Since the trauma model is a general model of
mental illness, I would have to master and reference the literatures
on all the major sections of DSM-IV-TR, in order to be
comprehensive. That is an impossible task. Fortunately, it is also
an irrelevant task. The purpose of the book is to outline the model
and the specific scientific predictions that follow from it, then
describe the principles of trauma therapy. I have therefore decided
not to be exhaustive in my referencing of the content of psychiatry.
The reader can consult any of the major comprehensive textbooks of
psychiatry for this content. For an inventory of measures relevant
to the predictions of the trauma model, I refer the reader to the
Handbook of Psychiatric Measures (Pincus, Rush, First, and McQueen,
2000).
The references in this book are illustrative only. I have used my
own published research to illustrate some points because I am
familiar with it, and because it was carried out within the trauma
model. Particular data are used only to illustrate the logic of the
model, not to prove it.
The trauma model is constructed to be falsifiable. Therefore it
could be wrong. That is how it is with scientific models.
Ideological objections to the model are irrelevant. What counts are
the data. There will be no single crucial experiment. The
predictions of the trauma model potentially lead to numerous Ph.D.
theses and research publications. Only after a body of data has
accumulated will the theory be either proven or rejected. The most
likely scientific outcome is that a bit of both will occur; the
theory will be proven, but modifications will be required.
The origins of the trauma model are in my work with comorbid
patients over the last twenty-one years. They are my teachers. I
thank them for presenting the problem in such poignant and
compelling form. I thank also the many other professionals who have
taken trauma seriously as a theme in psychiatry. The trauma model as
I have constructed it draws on the work of many different people. If
there is to be a paradigm shift in psychiatry, it will be due to the
collective work of many individuals. My task here is to present a
unified, testable summation of this collective effort.
In Schizophrenia: an Innovative Approach to Diagnosis and Treatment,[15] Ross determines that some patients diagnosed with schizophrenia have symptoms related to dissociative identity disorder.[16]
The family conditions during infancy are at present considered virtually irrelevant in the psychiatric profession.[17] According to some critics, the goal of modern psychiatric treatment is not to understand how parents could have contributed to the problem or how it can be resolved by improving the relationship. The objective is how to reduce the burden of a psychotic crisis for the family through medication of the disturbed individual. As two trauma researchers have put it, "the ideology of biological reductionism" in psychiatry is "to exonerate the family."[18]
In 2006 a UK researcher and a New Zealand clinical psychologist presented a meta-analysis of schizophrenia studies[19] to psychiatric conferences which they claimed demonstrated that the prevalence of physical and sexual abuse in the histories of those with schizophrenia is very high and is being under-studied.
The researchers admit that not all schizophrenics suffered trauma, but they believe "the level of actual abuse may be an important difference". While conceding that genetics may still be a causative risk factor they maintain "other evidence shows that genes alone do not cause the illness." The review caused considerable debate[20][21]
In the field of criminology, Lonnie Athens developed a theory of how a process of brutalization by parents or peers that usually occurs in childhood results in violent crimes in adulthood. Richard Rhodes' Why They Kill describes Athens' observations about domestic and societal violence in the criminals' backgrounds. Both Athens and Rhodes reject the genetic inheritance theories.[22]
Other criminologists such as Jonathan Pincus and Dorothy Otnow Lewis believe that, although it is the interaction of childhood abuse and neurological disturbances that explains murder, virtually all of the 150 murderers they studied over a 25-year period had suffered severe abuse as children. Pincus believes that the only feasible remedy for crime would be the prevention of child abuse.[23]
See also
EE Meditation, Shaman + Integrated Soul Personality, Fragmentation, MPD + DID, Psychology; Pt 1 of 3 There is in every person the possibility of an integrated Soul Personality. However,...
EE Meditation, Shaman + Integrated Soul Personality, Fragmentation, MPD + DID, Psychology; Pt 2 of 3 There is in every person the possibility of an integrated Soul Personality. However, normally the average person is split to a greater or lesser degree, dependent upon the amount of pain, trauma and undigested stress in their lives and dependent upon the amount of work they have done to integrate their personalities by means of therapy and meditation. Therapy and psychology allow intellectual appreciation of the problem in ourselves and others. It takes meditation to heal the splits and integrate the separated selves.
EE Meditation, Shaman + Integrated Soul Personality, Fragmentation, MPD + DID, Psychology; Pt 3 of 3 There is in every person the possibility of an integrated Soul Personality. Colin Ross (Ross, 1997) lists 11 dissociative features of the Shamen work, and relates each to Dissociative Identity Disorder or Splitting. These parallelisms are worth mentioning here, as they further ground the experiences of Split patients in a milieu that is pathological by reference to the abilities of Shamen which are integrated and real:
EE Meditation and the Kundalini Kriyas grounding Multiple Personalities, DID + MPD This is the second article after an Introduction on Split Personality using Shamen to illustrate the concept...
Myth Meditation Analysis of King Kong, Lord Of The Rings, Beauty + The Beast Indicating DID + MPD The movie of King Kong is an elaborate allegory of spiritual evolution so we can understand...
References
- ^ Cassidy, J., & Shaver, P., (Eds). (1999) Handbook of Attachment: Theory, Research, and Clinical Applications. Guilford Press, NY
- ^ Main, M. & Hesse, E. (1990). "Parents' unresolved traumatic experiences are related to infant disorganized attachment status: Is frightened and/or frightening parental behavior the linking mechanism?" In Greenberg, M., Cicchetti, D., and Cummings, M. (Eds.), Attachment In The Preschool Years: Theory, Research, and Intervention. Chicago: University of Chicago Press.
- ^ Lilienfeld, Scott (1995). "Will the real pseudoscientists please stand up?". Skeptical Inquirer November/December: 45.
- ^ Hahlweg, K; et al. (2000). "Familienbetreuung als verhaltenstherapeutischer Ansatz zur Ruckfallprophylaxe bei schizophrenen Patienten", in M. Krausz, D. Naber (eds.) Integrative Schizophrenietherapie. Freiburg: Karger.
- ^ [1] - article on Theodore Lidz
- ^ associazionesilvanoarieti.org - page on Arieti (mostly in Italian)
- ^ Kendler, K; et al. (2000). "Childhood sexual abuse and adult psychiatric and substance use disorders in women". Archives of General Psychiatry 57 (10): 953�959. doi:10.1001/archpsyc.57.10.953. PMID 11015813.
- ^ Mullen, P. E.; et al. (1993). "Childhood sexual abuse and mental health in adult life". British Journal of Psychiatry 163: 721�32. doi:10.1192/bjp.163.6.721. PMID 8306113.
- ^ Davies, Emma; Jim Burdett (2004). "Preventing 'schizophrenia': creating the conditions for saner societies" in Read et al., Models of Madness. Routledge.
- ^ Piper, August (1998). "Multiple personality disorder: witchcraft survives in the twentieth century". Skeptical Inquirer May/June.
- ^ Arieti, Silvano (1994). Interpretation of Schizophrenia. Aronson. p. 197.
- ^ [2] - article by Lloyd deMause
- ^ [3] - John Modrow�s book
- ^ [4] - Colin Ross' web site
- ^ Colin, Ross (2004). Schizophrenia: An Innovative Approach to Diagnosis and Treatment. Haworth Press.
- ^ [5] Ross� book on schizophrenia
- ^ Johnstone, Lucy (1993). "Family management in "schizophrenia": its assumptions and contradictions". Journal of Mental Health 2: 255�69. doi:10.3109/09638239309003771.
- ^ Aderhold, Volkmar; Evelyn Gottwalz (2004). Family therapy and schizophrenia: replacing ideology with openness� in Read et al., Models of Madness. Routledge.
- ^ Read J, van Os J, Morrison AP, Ross CA (November 2005). "Childhood trauma, psychosis and schizophrenia: a literature review with theoretical and clinical implications". Acta Psychiatr Scand 112 (5): 330�50. doi:10.1111/j.1600-0447.2005.00634.x. PMID 16223421.
- ^ "Media report of sexual abuse as cause of schizophrenia". http://www.scienceagogo.com/news/20060514024158data_trunc_sys.shtml. Retrieved 2009-04-15.
- ^ "Maudsley debate on sexual abuse as a cause of schizophrenia". http://www.iop.kcl.ac.uk/podcast/?id=208&type=item. Retrieved 2009-04-15.
- ^ Rhodes, Richard (2000). Why They Kill: The Discoveries of a Maverick Criminologist. Vintage. ISBN 0375402497.
- ^ Pincus, Jonathan (2002). Base Instincts: What Makes Killers Kill. W.W. Norton & Company. ISBN 039305022X.
External links
- Alice-Miller.com - According to Miller, the "forbidden issue" is the parental role in mental disorders
- LaingSociety.org - The Society for Laingian Studies, R.D. Laing (1927�1989)
- MosherSoteria.com - Loren Mosher, MD, (1933�2004)
- Prof J.J. Freyd's Betrayal Trauma Theory Home Page at the University of Oregon
- Psychohistory.com - The Institute for Psychohistory
- Rossinst.com - Home page of the Ross Institute for Psychological Trauma